Unexplained Pain, No Caries, No Trauma — CBCT Solved It at 75 Microns
A 29-year-old with anterior maxillary pain and a palatal swelling that defied clinical and 2D radiographic diagnosis. High-resolution CBCT revealed a rare developmental anomaly invisible on conventional imaging — and changed the treatment plan entirely.
 Dr Aditya Patney
Dr Aditya Patney
A 29-year-old male was referred with pain in his upper left front teeth that had been present for several days. There was a visible palatal swelling, but clinically nothing added up — no caries, no restorations, no history of trauma. The tooth looked healthy.
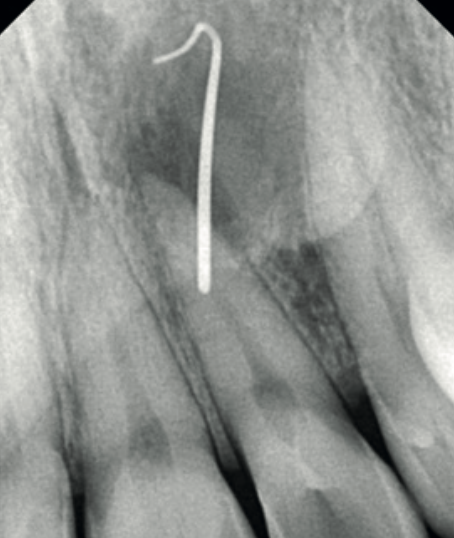
A periapical radiograph of the upper left lateral incisor (UL2) was taken with sinus tracing through the palatal swelling. It was inconclusive. The 2D image could not establish a diagnosis. The referring clinician was stuck.

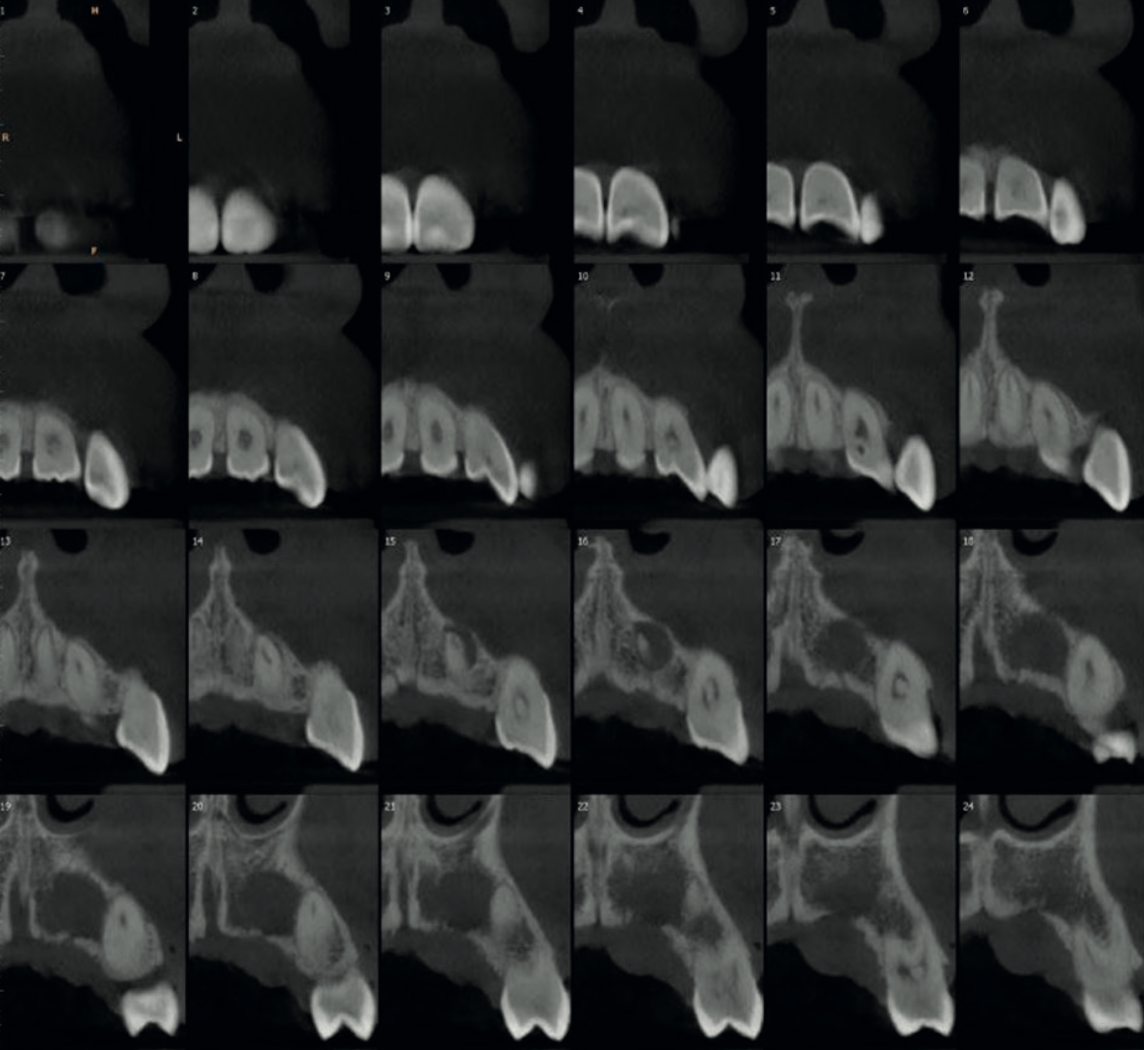
A high-resolution CBCT scan of the anterior maxilla was performed using the Carestream CS 9600 at its maximum resolution — a voxel size of just 75 microns. At this resolution, the scan reveals anatomy that is invisible on standard periapical radiography and would be missed on lower-resolution 3D scans.
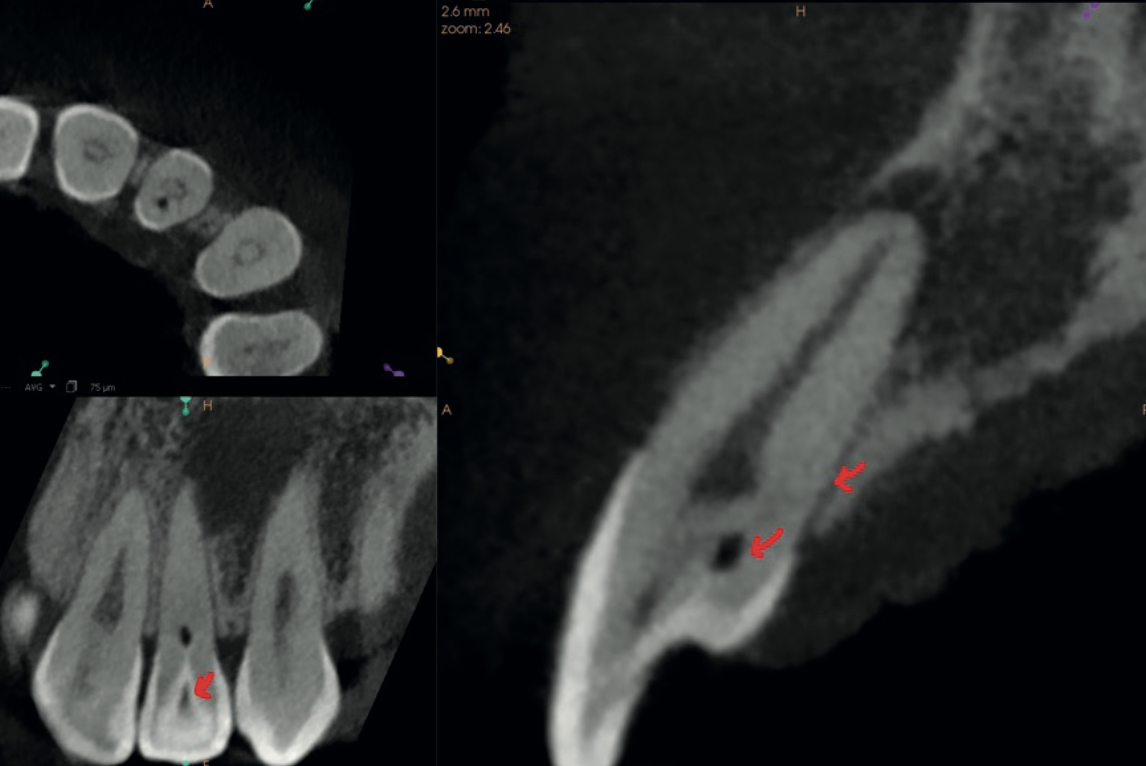
The CBCT immediately revealed the diagnosis: Oehler's Type III Dens Invaginatus — the most severe form of a rare developmental anomaly where enamel folds inward through the tooth all the way to the root apex. The invagination communicated laterally with the periodontal ligament through a pseudo-foramen via a faintly visible palatal extension. An open apex was also identified.
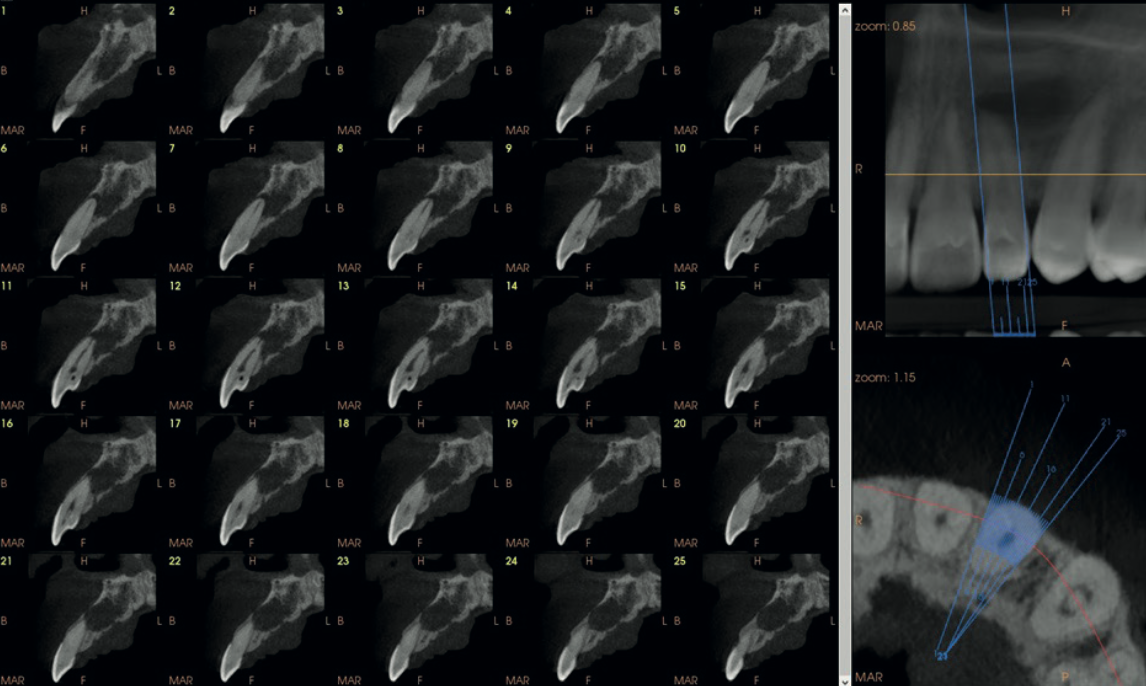
The scan also showed focal calcification in the coronal third of the main root canal, with the canal space dilated in the middle third and well-visualised calibre in the remainder. Thin cross-sectional slices mapped the full morphological complexity of the tooth.
Dens Invaginatus — Oehler's classification
Dens Invaginatus is a developmental malformation where the outer surface of the tooth folds inward during formation. It most commonly affects maxillary lateral incisors and ranges from mild (Type I) to severe (Type III). It is notoriously difficult to diagnose on 2D imaging because the invagination overlaps with normal anatomy on a periapical radiograph.
The CBCT also revealed a well-defined periapical lesion measuring 1.3 cm × 1.0 cm × 1.3 cm in the UL2–UL3 region. There was mild expansion and thinning of the cortical bone, with significant focal erosion of the palatal bone adjacent to UL3 and contiguous soft tissue thickening — explaining the palatal swelling that had prompted the referral in the first place.
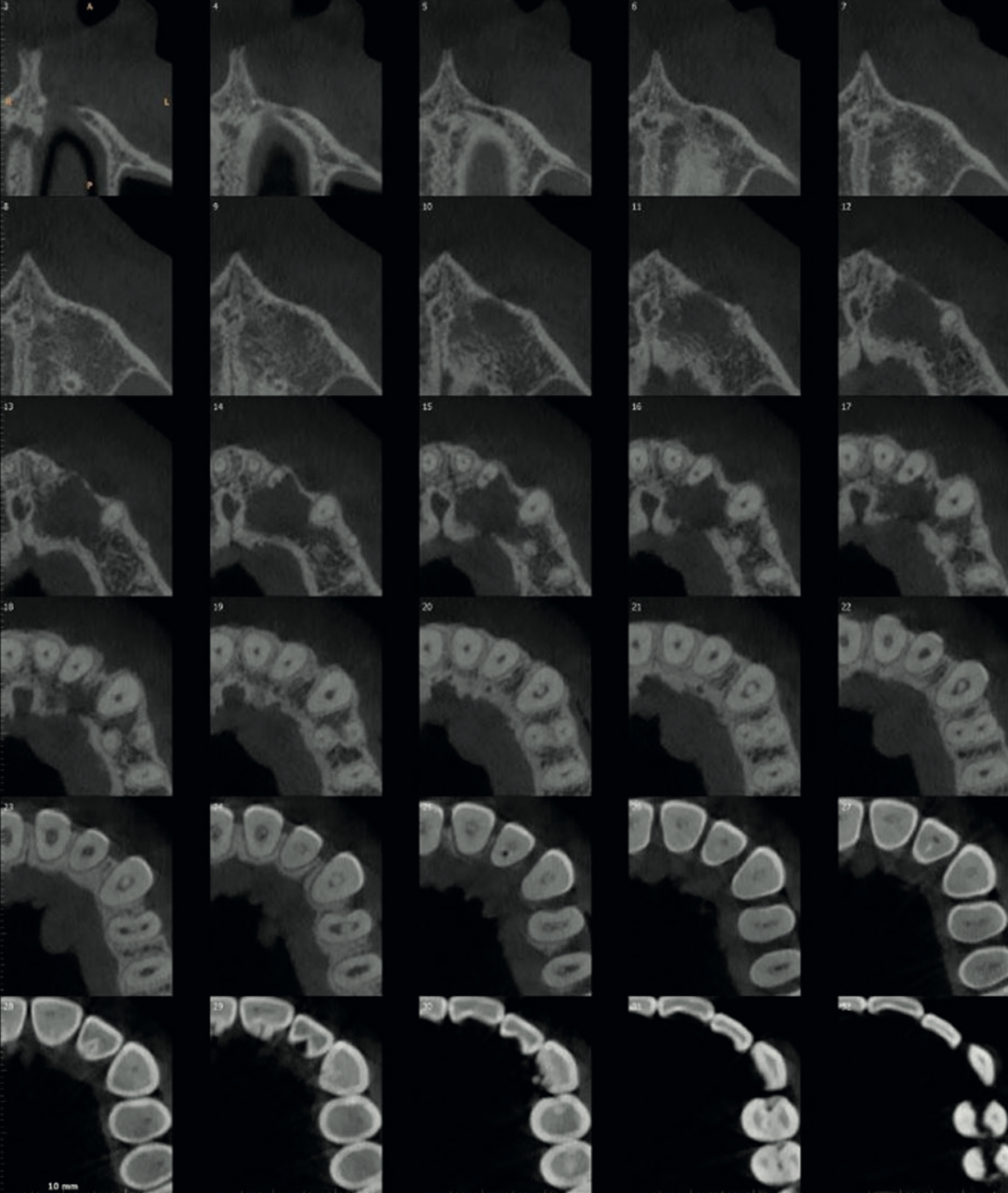
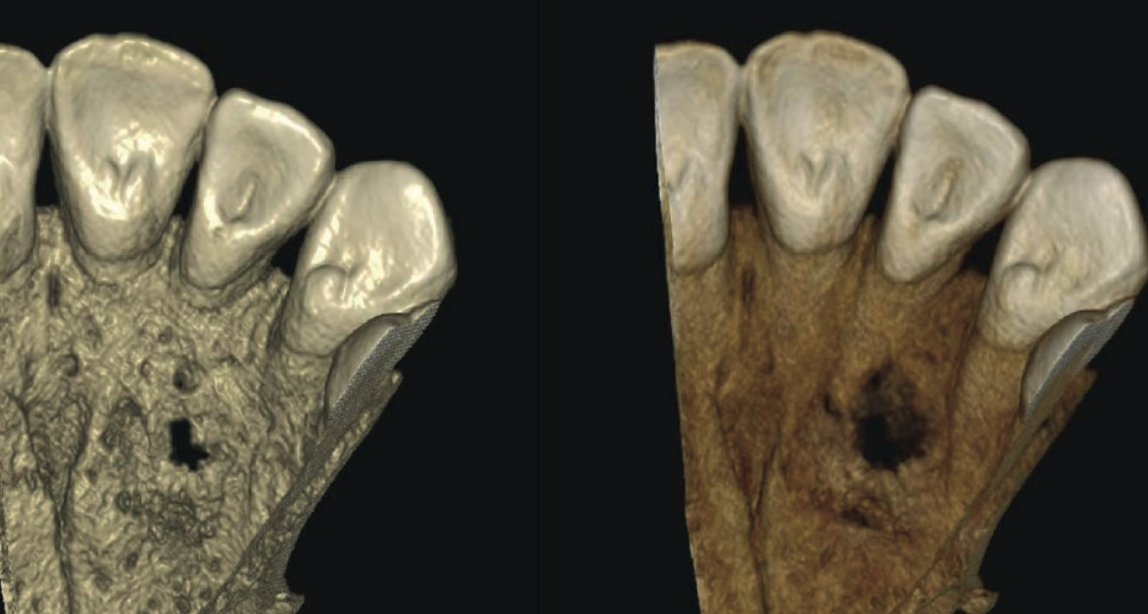
The diagnosis was clear: a chronic periapical lesion — periapical cyst with secondary infection — involving the UL2–UL3 region, caused by the Type III Dens Invaginatus in UL2. The recommended treatment was endodontic intervention directed at UL2, with post-treatment follow-up imaging to monitor the aberrant anatomy.
This case underscores the importance of prudent CBCT protocol selection and careful reading of the scan volume. The invagination was barely perceptible even at the highest possible resolution — at a standard voxel size, it may well have been missed entirely.
— Based on the clinical conclusions of Dr Aditya PatneyWhen 2D radiography draws a blank, CBCT is the next step. Pain with no visible cause on a periapical radiograph is a recognised indication for 3D imaging. In this case, the periapical film showed nothing diagnostically useful — the CBCT provided the complete answer.
Resolution matters. The CS 9600's 75-micron voxel size was critical here. The dens invaginatus was barely perceptible even at this resolution. A lower-resolution scan may have missed the finding entirely. When you suspect subtle anatomy, high-resolution protocols make the difference.
Dens Invaginatus is rare but clinically significant. It most commonly affects maxillary lateral incisors and can cause unexplained pulpal and periapical pathology. If conventional imaging cannot explain anterior pain in a seemingly healthy tooth, consider this diagnosis — and reach for the CBCT.
Systematic CBCT reading is a learned skill. Subtle findings on a 3D scan are easy to miss if you are not trained to look for them. Our CBCT Level 2 Reporting Course teaches structured, systematic interpretation — so you see what's there, not just what you expect.

Carestream CS 9600
The CS 9600's 75-micron voxel size — the highest resolution in the Carestream CBCT range — was critical in this case. Five imaging modes in a single unit: panoramic, cephalometric, CBCT, facial scan, and optional tomosynthesis.
View CS 9600 specifications →Could you confidently interpret a finding this subtle on a CBCT scan?