How CBCT Revealed a Hidden Canal That 2D X-Rays Missed
A routine endodontic case became anything but routine when 3D imaging uncovered a second palatal canal invisible on periapical radiography — changing the treatment plan entirely.
 Dr Roberto Aza
Dr Roberto Aza
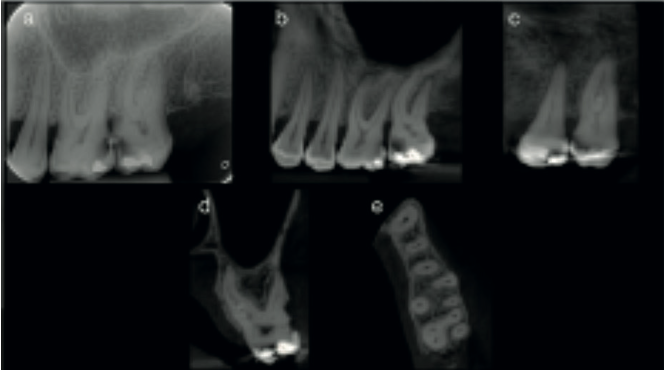
A 44-year-old male patient was referred with pain in his upper left posterior region. Initial periapical radiographs showed extensive decay affecting both the upper left first and second molars (UL6 and UL7). Clinical testing — palpation, percussion, and sensibility — confirmed symptomatic irreversible pulpitis in the UL7.
The problem: the standard periapical X-ray could not clearly show the root canal anatomy of this tooth. Maxillary second molars are well known for anatomical variability, and a 2D image simply does not give you enough information when you suspect something unusual is going on inside the roots.
In line with the 2025 AAE/AAOMR joint position statement, a limited field-of-view CBCT scan was justified. The guidelines are clear: when conventional radiographs are inconclusive and complex canal anatomy is suspected, 3D imaging is indicated — particularly when the additional information will directly influence the treatment plan.
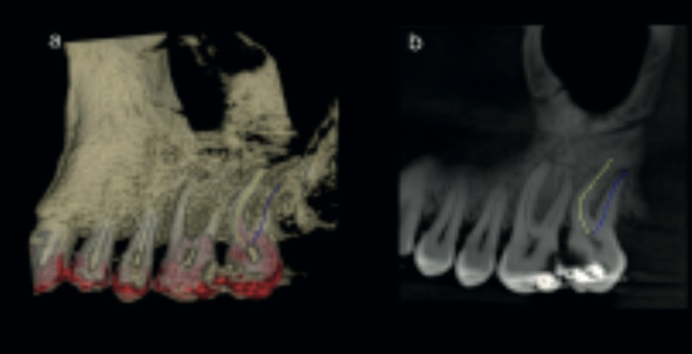
The CBCT scan immediately revealed what the periapical film could not: two separate canals in the palatal root. This is an uncommon but clinically significant finding in maxillary second molars. Without 3D imaging, the second palatal canal would almost certainly have been missed.
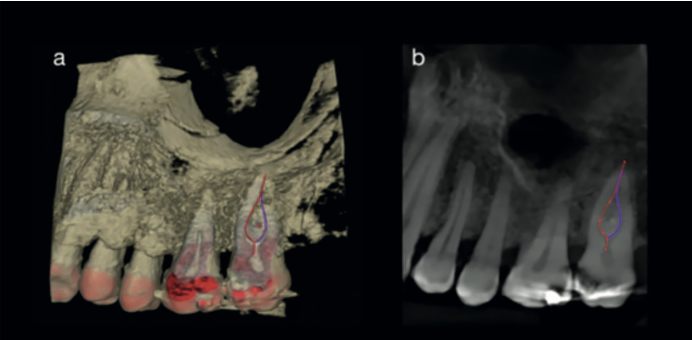
Virtual treatment planning was then carried out using 3D imaging software with a root canal tracing tool. This allowed the clinician to map the entire canal system before touching the tooth — assessing morphology, planning the access cavity, and reducing the risk of perforation, missed canals, or instrument separation.
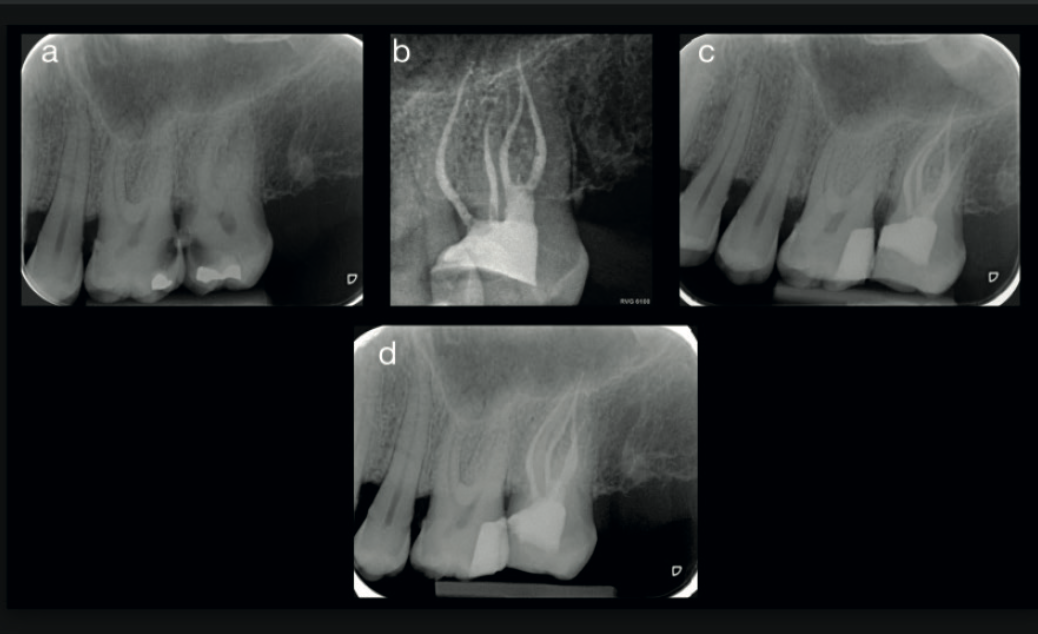
Endodontic treatment was completed under magnification. Intraoperative findings confirmed exactly what the CBCT had shown: two distinct canals in the palatal root. All canals were instrumented, cleaned, and obturated.
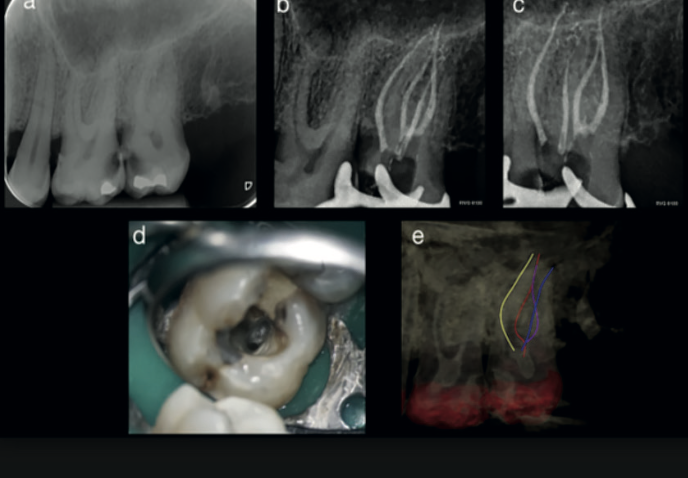
Post-operative radiographs showed satisfactory obturation of all identified canals. At two-year follow-up, the tooth remained asymptomatic with healthy periapical tissues — a successful outcome that would have been unlikely had the second palatal canal been missed.
The 3D imaging completely changed the treatment plan. Without the CBCT, the second palatal canal would almost certainly have been missed — and that missed canal is precisely the kind of thing that leads to persistent symptoms and re-treatment.
— Based on the clinical findings of Dr Roberto AzaMissed canals remain a leading cause of endodontic failure. If your periapical radiograph does not clearly show the canal system, a limited FOV CBCT scan can reveal anatomy that 2D imaging simply cannot. The 2025 AAE/AAOMR guidelines support this approach.
Virtual treatment planning reduces procedural risk. Root canal tracing software lets you map the canal system before you start, reducing the chance of perforation, missed anatomy, or instrument separation.
Limited FOV keeps radiation exposure low. You do not need a full-volume scan for endodontic diagnosis. A small field of view centred on the tooth of interest gives you the diagnostic information you need while keeping dose to a minimum — fully aligned with ALARA principles.
Confident CBCT reporting is a skill worth developing. If you own a CBCT and want to report your own endodontic scans with confidence, our CBCT Level 2 Reporting Course covers structured report writing, dataset manipulation, and clinical decision-making — led by a Consultant Dental Radiologist.
Carestream CBCT Systems
360 Visualise supplies and supports the full Carestream CBCT range — including the CS 8200 and CS 9600 — with limited FOV modes ideal for endodontic diagnosis. Installed, configured, and supported from day one.
Compare CBCT systems →Want to develop your CBCT reporting skills for endodontic cases like this?