The Implant Scan That Found Carotid Artery Calcifications
A routine pre-implant CBCT revealed far more than bone levels. A large field of view uncovered five incidental findings — including calcified atheromatous plaques suggesting stroke risk. This case shows why reporting matters as much as scanning.
 Prof. Ingrid Różyło-Kalinowska
Prof. Ingrid Różyło-Kalinowska
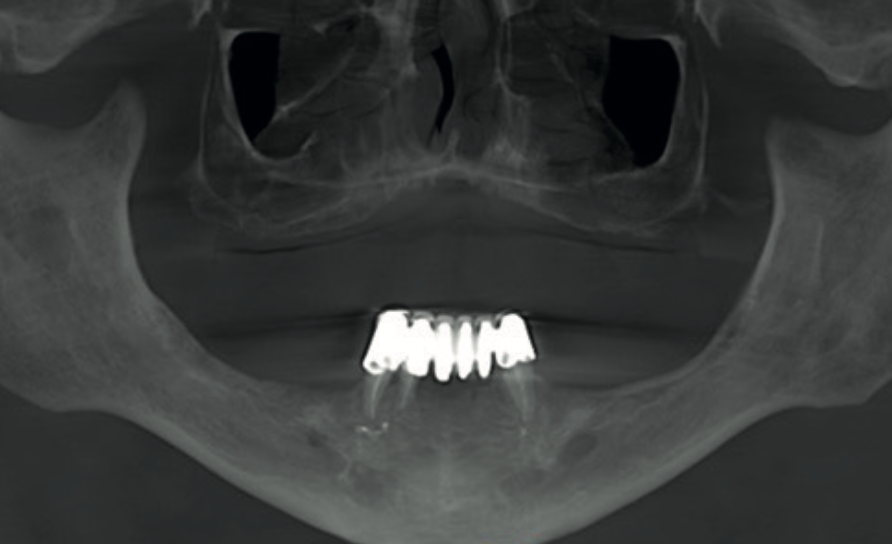
A 65-year-old male with an unremarkable medical history was referred for a CBCT scan before planning implant placement. He was fully edentulous in the upper jaw. In the mandible, only three teeth remained — the lower right canine, lower right lateral incisor, and lower left canine — all endodontically treated and supporting a fixed bridge.
The referral was straightforward: assess bone levels for dental implants. But the scan that came back told a much bigger story.
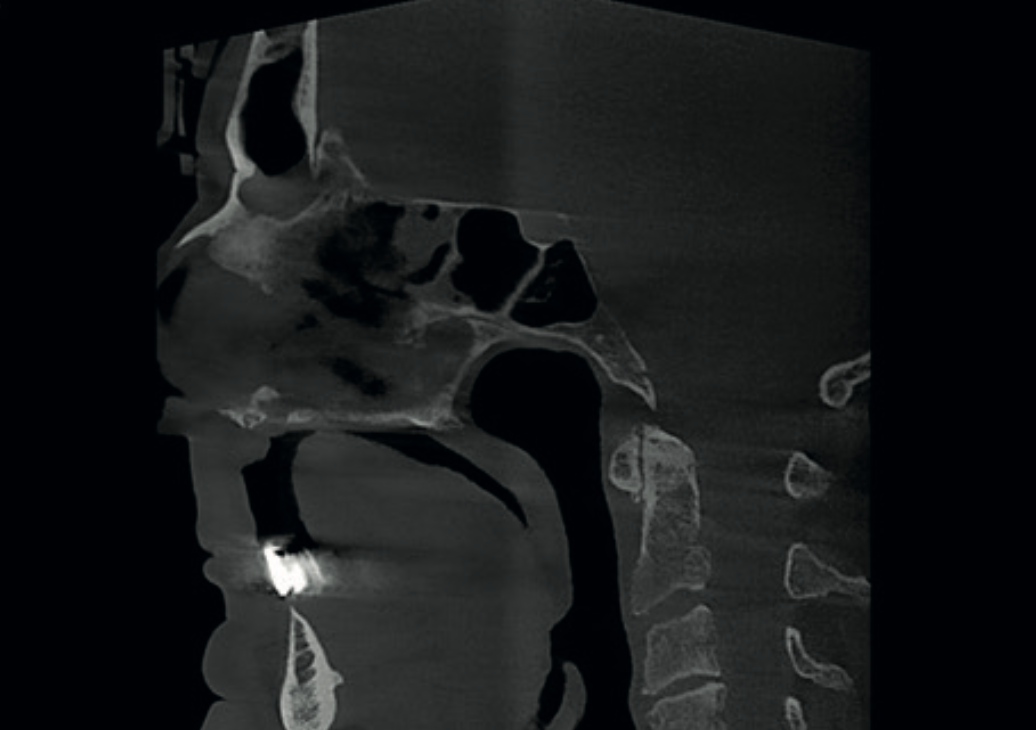
A large field-of-view CBCT scan (16×17 cm) was acquired using the Carestream CS 9600. This captured not just the jaws, but the entire maxillofacial region — sinuses, cervical spine, and the course of the carotid arteries.
The implant assessment itself was relatively straightforward. Cross-sectional views confirmed that the maxillary alveolar bone was severely atrophic — the residual ridge height was too small to provide sufficient anchorage for implants. Implant placement was only feasible in the posterior mandible, though bone quality there showed some rarefication that could compromise primary stability.
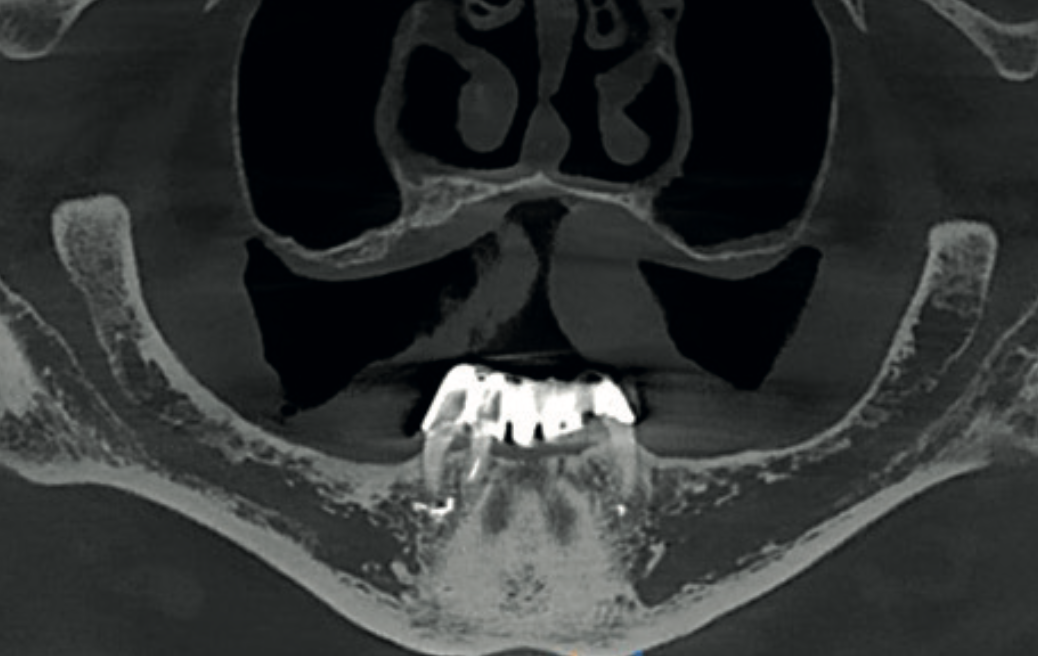

So far, a straightforward implant report. But with a 16×17 cm field of view, the reporting responsibility does not stop at the alveolar bone. Every structure captured in the volume must be evaluated and reported. That is where this case became anything but routine.
Systematic evaluation of the full CBCT volume revealed five clinically significant incidental findings — none of which were related to the original implant referral, but all of which required documentation, and several demanded further investigation.
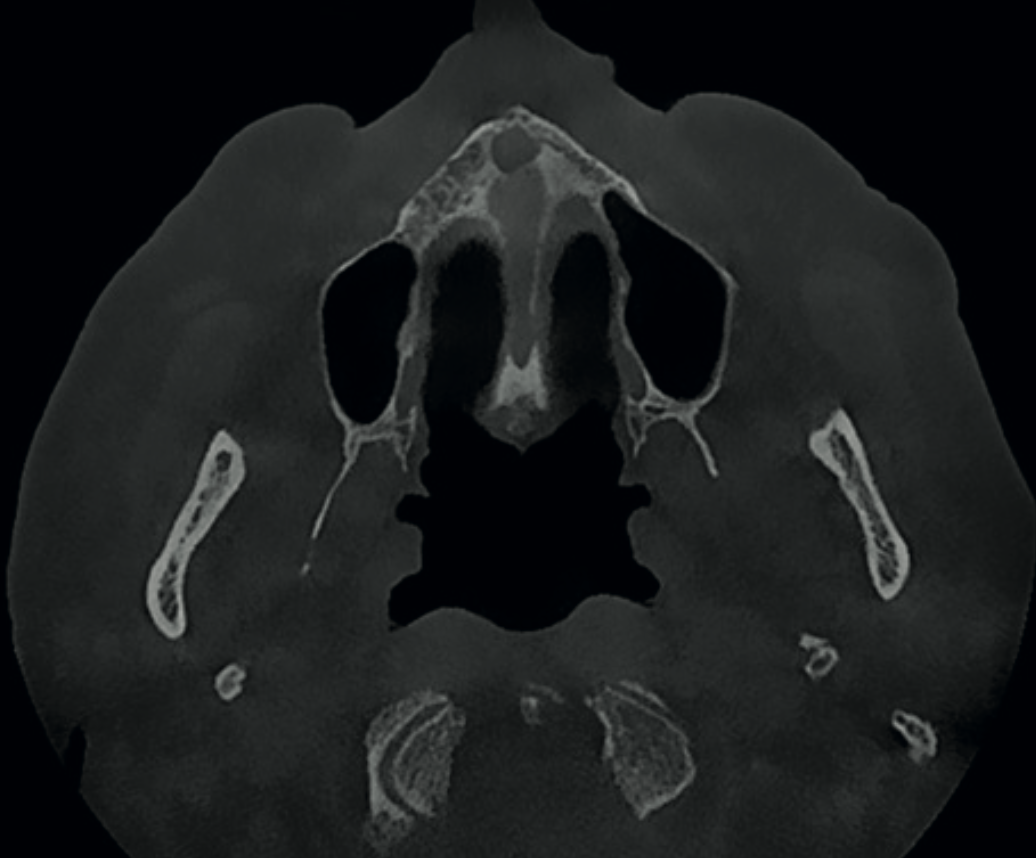
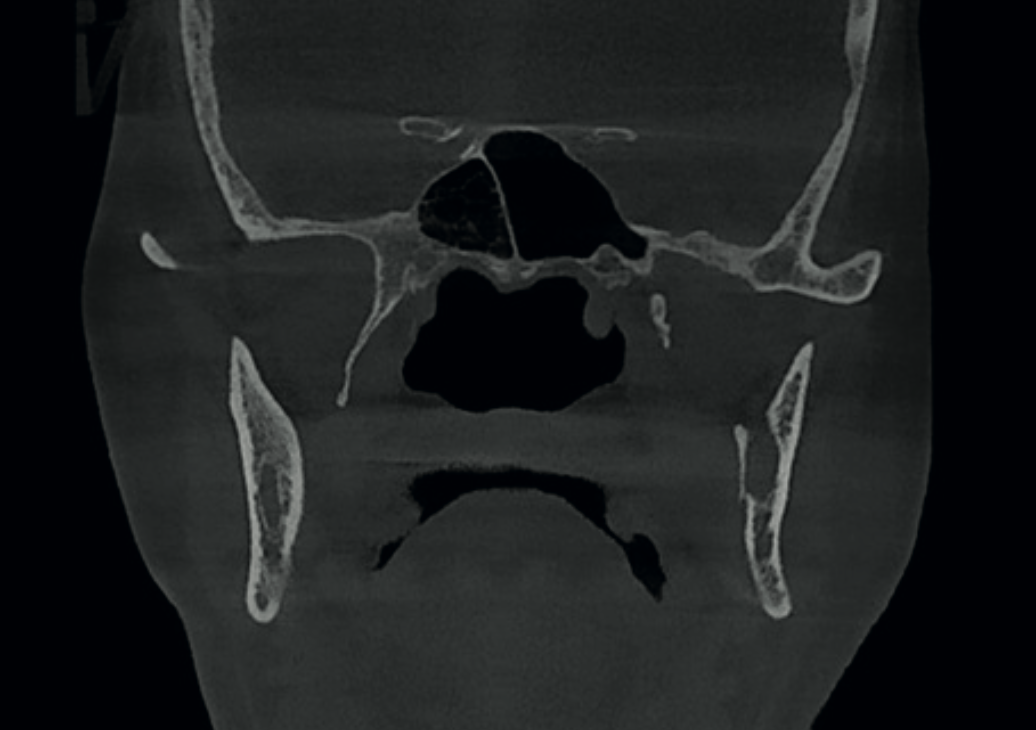
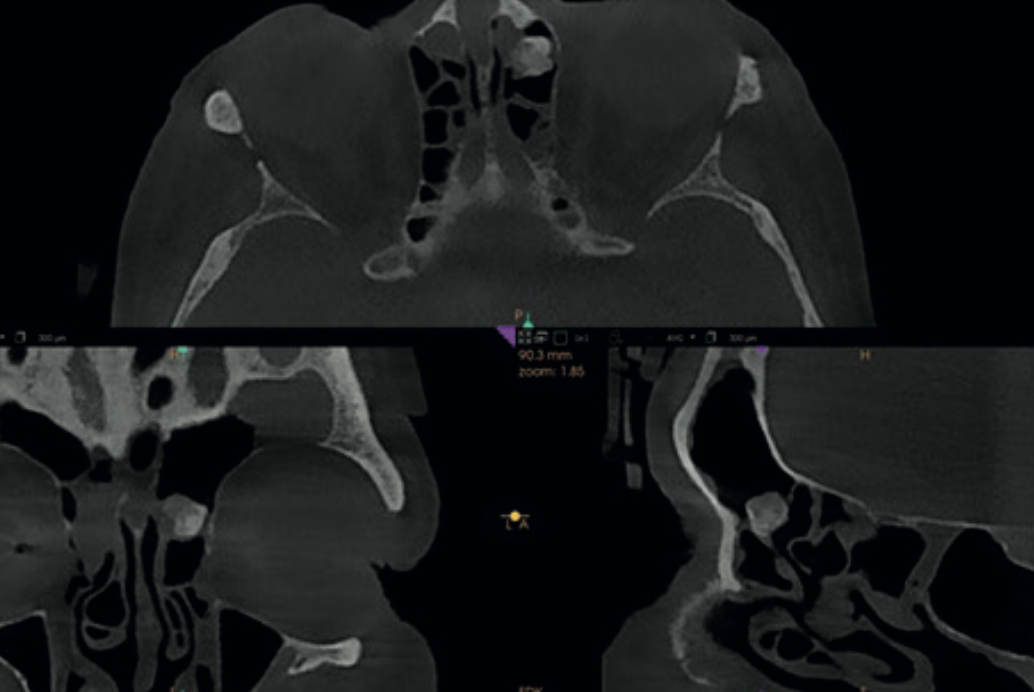
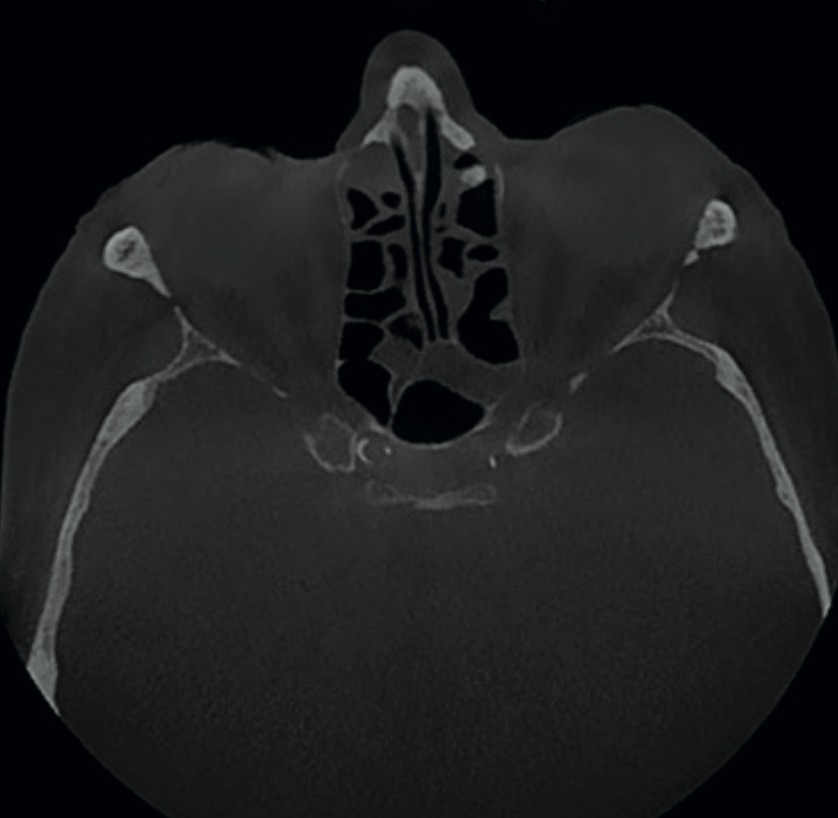
Calcified atheromatous plaques were identified at multiple locations along the carotid arteries — both in the neck and in the intracranial sections of the internal carotids. This is a significant finding that suggests advanced atherosclerosis and may indicate increased stroke risk.
Without early identification, carotid artery calcifications can progress silently. This patient required onward referral for Doppler ultrasound examination of the carotid arteries — a diagnostic step that would never have been triggered without thorough evaluation of the CBCT volume.

The eye sees what the mind is prepared to comprehend. In radiology, perception is not just about vision — it is about training, experience, and expectation. If you are not trained to recognise incidental findings, you will not see them — even when they are right in front of you.
— Prof. Ingrid Różyło-Kalinowska, referencing the principle attributed to Henri BergsonIf you scan it, you must report it. When a large FOV CBCT is acquired, the practitioner is responsible for evaluating and reporting every structure captured — not just the area of clinical interest. Incidental findings can have serious medical consequences, including stroke risk indicators like carotid artery calcifications.
Use the smallest field of view that answers the clinical question. ALARA principles apply directly to FOV selection. A limited FOV for an implant assessment in a single quadrant avoids exposing the patient to unnecessary radiation and avoids capturing anatomy you may not be trained to interpret.
Know the limits of your reporting competence. Dental curricula do not routinely cover interpretation of the cervical spine, carotid arteries, or paranasal sinuses. If you are using large FOV CBCT, you need either the reporting skills to evaluate these structures or a referral pathway to a specialist radiologist who can.
Structured reporting training changes what you can see. Our CBCT Level 2 Reporting Course is designed to build exactly this capability — led by a Consultant Dental Radiologist, covering structured report writing, dataset manipulation, and knowing when to refer. Limited to 15 delegates for direct access to your trainer.
Carestream CS 9600
The CS 9600 offers multiple field-of-view options from 5×5 cm focused scans up to the 16×17 cm full maxillofacial volume used in this case. Flexible FOV selection means you scan what you need — no more, no less.
View CS 9600 specifications →Are you confident you could identify incidental findings like these on a large FOV scan?