A Calcified Canal, a Failed Access, and Dynamic Navigation to the Rescue
When the first attempt to locate a calcified canal went wrong, high-resolution CBCT mapped the problem and dynamic navigation guided a minimally invasive retreatment — with complete periapical healing at 12 months.
 Dr Roberto Aza
Dr Roberto Aza
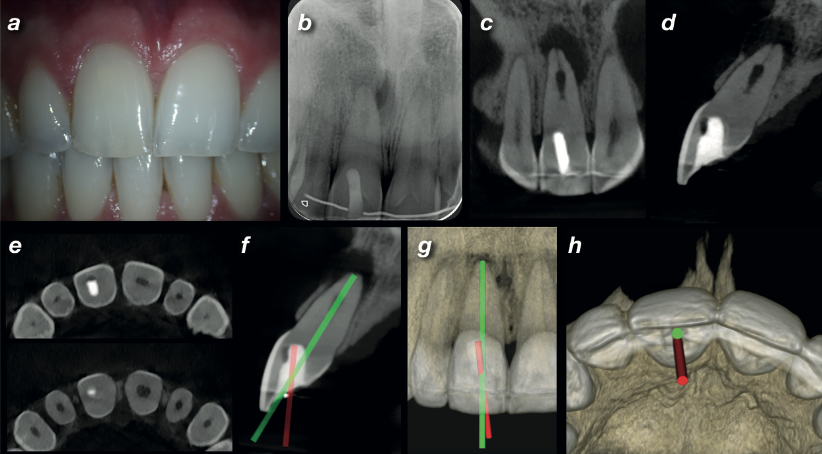
A 26-year-old male was referred after his dentist was unable to locate the root canal in the upper right central incisor (UR1) during endodontic treatment. The tooth was tender to palpation and percussion, with slight discolouration compared to the opposite side — a classic sign of pulp canal obliteration following earlier trauma.
The periapical radiograph told a worrying story: a deviated access cavity from the first attempt, a calcified root canal, internal resorption, and a periapical radiolucency. The initial treatment had gone off course — the access was angled in the wrong direction, and the canal had never been located.
The AAE classifies endodontic treatment of obliterated canals as a high level of difficulty. The risks are real: overextended access cavities, iatrogenic perforation, missed canals, file separation. Even with microscopes and ultrasonics, excessive dentine removal is common. This case needed a different approach.
A high-resolution CBCT scan was taken using the Carestream CS 8100 3D with a limited 5×5 cm field of view at 75-micron voxel size. The scan clearly showed the deviation of the initial access, the extent of the calcification, the internal resorption, and the periapical lesion with perforation of the buccal cortical plate.
Using the CBCT data, a "virtual endodontic guide" was designed — overlaying the correct drilling path onto the scan alongside the failed original access. The difference was immediately visible: the first attempt had been angled too far in one direction to ever reach the canal.
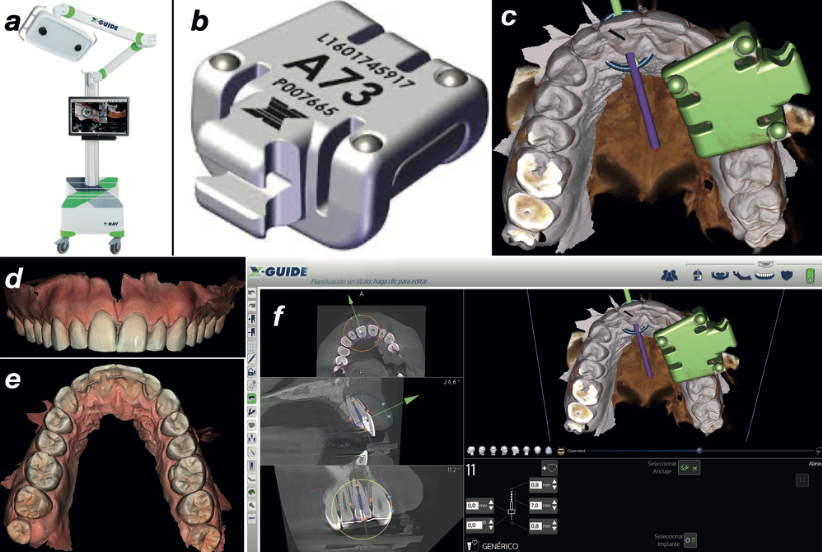
Non-surgical retreatment with dynamic navigation was indicated. The X-Guide system provides real-time visualisation of bur position, angle, and depth during the procedure — effectively turning the CBCT data into a live GPS for the handpiece.
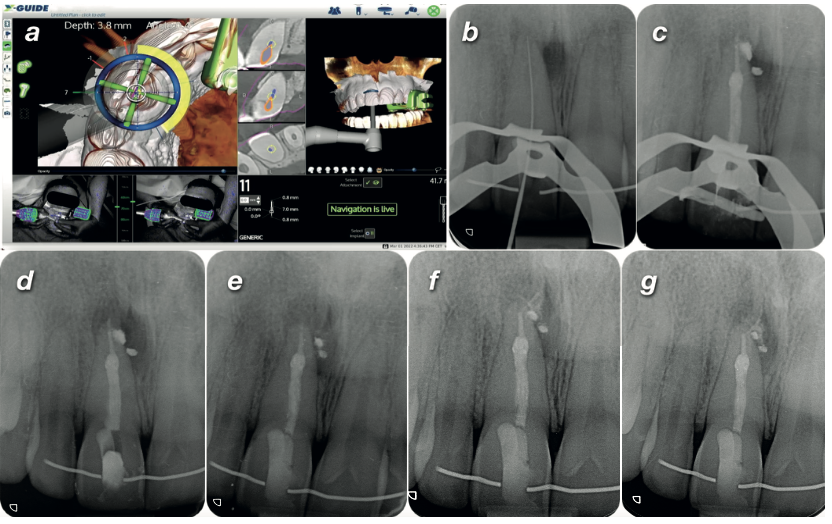
Under rubber dam isolation, the X-Clip was reinserted and the system calibrated. Live navigation guided a size #1 Munce bur along the planned drilling path until it reached the target depth. The canal was located successfully — confirmed by periapical radiograph.
The canal was instrumented, cleaned, and obturated using a warm vertical technique. The patient was referred back to his dentist for definitive restoration.
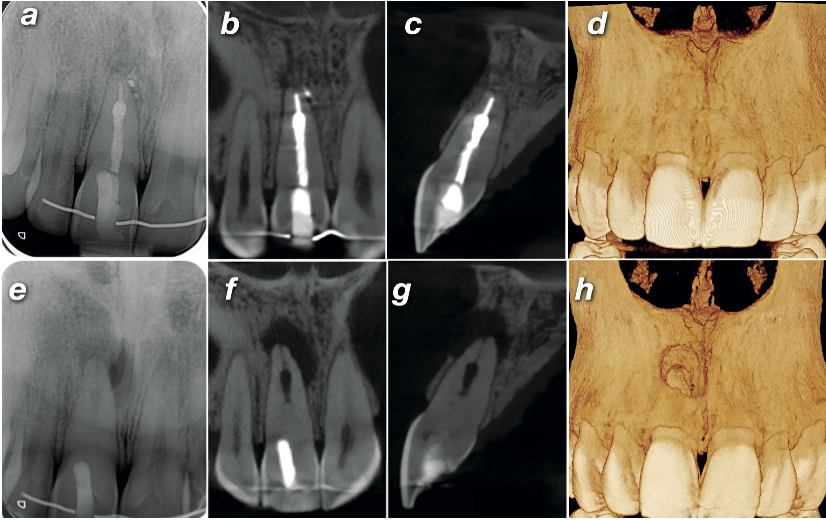
Follow-up radiographs at 1, 3, and 6 months showed no clinical symptoms and a steadily shrinking periapical radiolucency. At 12 months, a follow-up high-resolution CBCT confirmed complete healing of the periapical pathology — and volume rendering showed full regeneration of the buccal cortical plate that had been perforated at the time of diagnosis.
High-resolution CBCT is needed to make a correct diagnosis and an accurate treatment plan. In calcified canal cases, image quality is not a luxury — it is the difference between locating the canal and missing it entirely.
— Based on the clinical conclusions of Dr Roberto AzaCalcified canals are high-risk — and CBCT is essential. The AAE classifies obliterated canal treatment as high difficulty. Without 3D imaging, you are navigating blind. High-resolution CBCT at 75 microns mapped the calcification, the failed access, and the periapical pathology in this case — none of which were fully visible on the periapical radiograph.
Dynamic navigation turns CBCT data into a live surgical guide. By merging CBCT and intraoral scan data, the clinician planned the exact entry point, angle, and depth before touching the tooth — then followed that plan in real time during the procedure. The result was a minimally invasive access with no further deviation.
A limited FOV at maximum resolution is the right protocol for endodontics. The CS 8100 3D's 5×5 cm field of view at 75 microns delivered the resolution needed to see a calcified canal that would be invisible on a standard scan — while keeping radiation exposure to a minimum.
Confident CBCT interpretation is the foundation of guided workflows. Navigation technology is only as good as the scan it is built on — and the clinician's ability to read that scan. Our CBCT Level 2 Reporting Course builds the systematic interpretation skills that underpin every guided and navigated procedure.

Carestream CS 8100 3D
The CS 8100 3D combines panoramic, cephalometric, and CBCT imaging in a compact footprint. Its 75-micron high-resolution mode and 5×5 cm limited FOV make it ideal for endodontic diagnosis and guided workflow planning.
View Carestream CBCT range →Ready to build confidence in CBCT interpretation for complex endodontic cases?